The MedTech Career: What the Numbers Actually Say
Two device reps, same job title, same year. One tops out at $220K and one clears $600K. Neither is five times better at selling. What separates them is position on the adoption curve, not skill, and that reframes what sales coaching is actually for.
Two medical device reps. Same country, same year, same job title on the business card. One sells diagnostic imaging and tops out around $220,000. One sells spine and clears $600,000.
Neither of them is five times better at selling.
That is the finding underneath every number in this piece, and it is worth sitting with before we get to the mechanics. The MedTech commercial career has the highest floor in professional sales and a ceiling most people never touch. What separates the floor from the ceiling is not effort, not tenure and not credentials. It is position. And almost nobody manages a career, or coaches one, as if that were true.
We ranked the pay ladder in Same Job, Different Paycheck. This piece asks the harder question: what actually moves a rep from one rung to another.
The Ladder
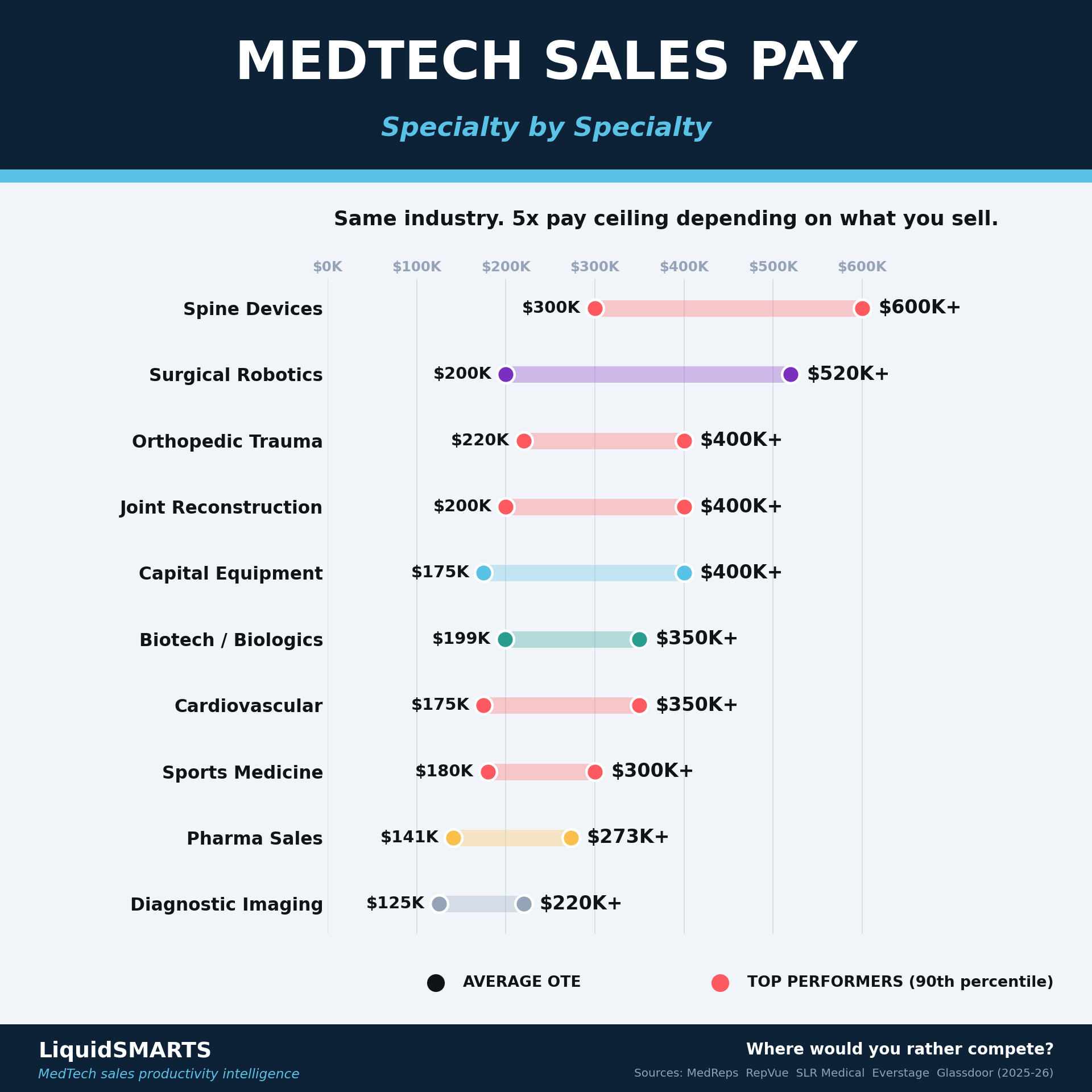
| Specialty | Average OTE | Top performers (90th) |
|---|---|---|
| Spine devices | $300K | $600K+ |
| Surgical robotics | $200K | $520K+ |
| Orthopedic trauma | $220K | $400K+ |
| Joint reconstruction | $200K | $400K+ |
| Capital equipment | $175K | $400K+ |
| Biotech / biologics | $199K | $350K+ |
| Cardiovascular | $175K | $350K+ |
| Sports medicine | $180K | $300K+ |
| Pharma | $141K | $273K+ |
| Diagnostic imaging | $125K | $220K+ |
Same industry. A 5x spread in the ceiling depending on what happens to be in the bag.
Widen the lens and MedTech holds up well against every other place you could sell.
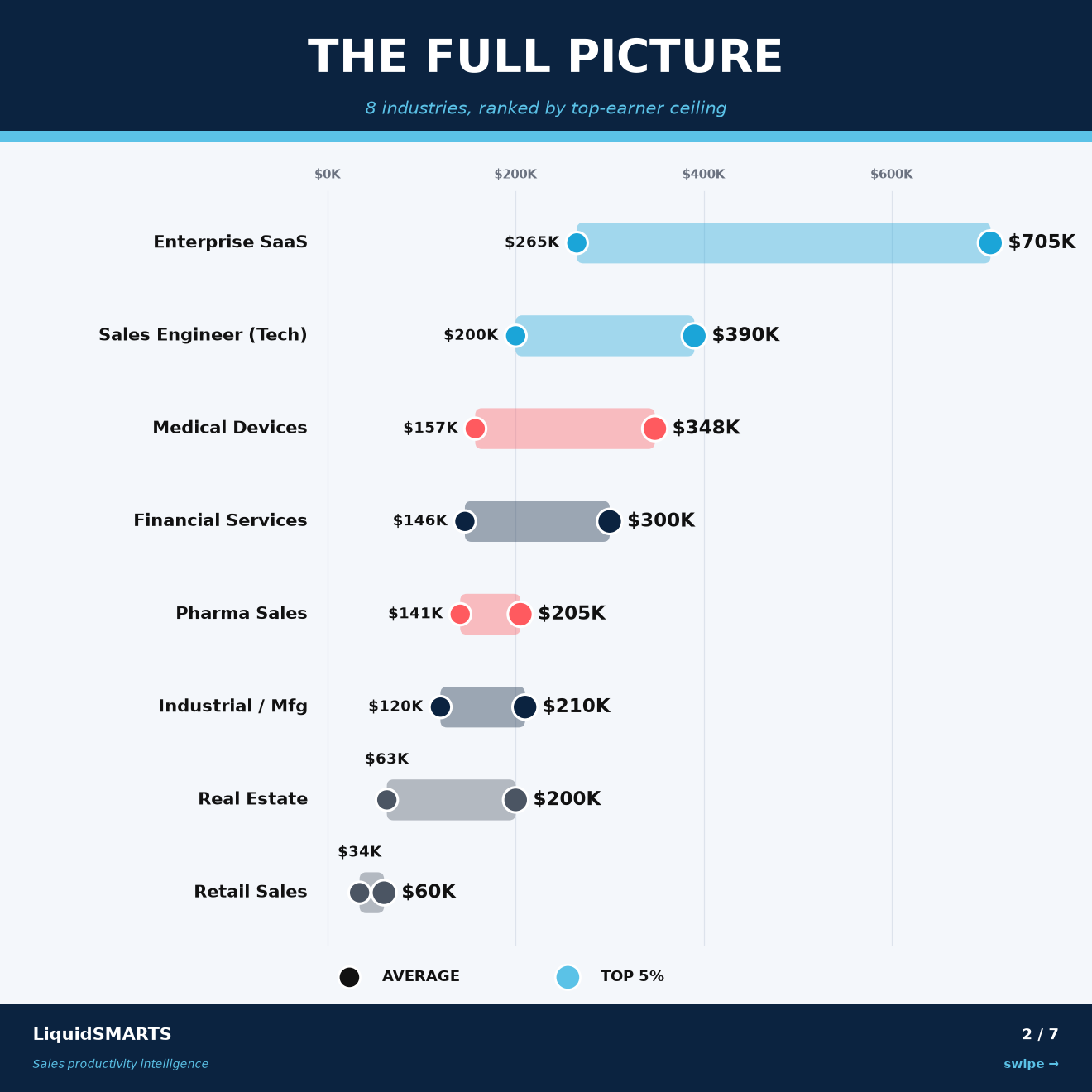
Enterprise SaaS has the higher ceiling. MedTech has the higher floor, and it does not require a computer science degree, a coastal zip code or a funding round to hold up.
Who Actually Sells
Now the number that should worry every commercial leader reading this.
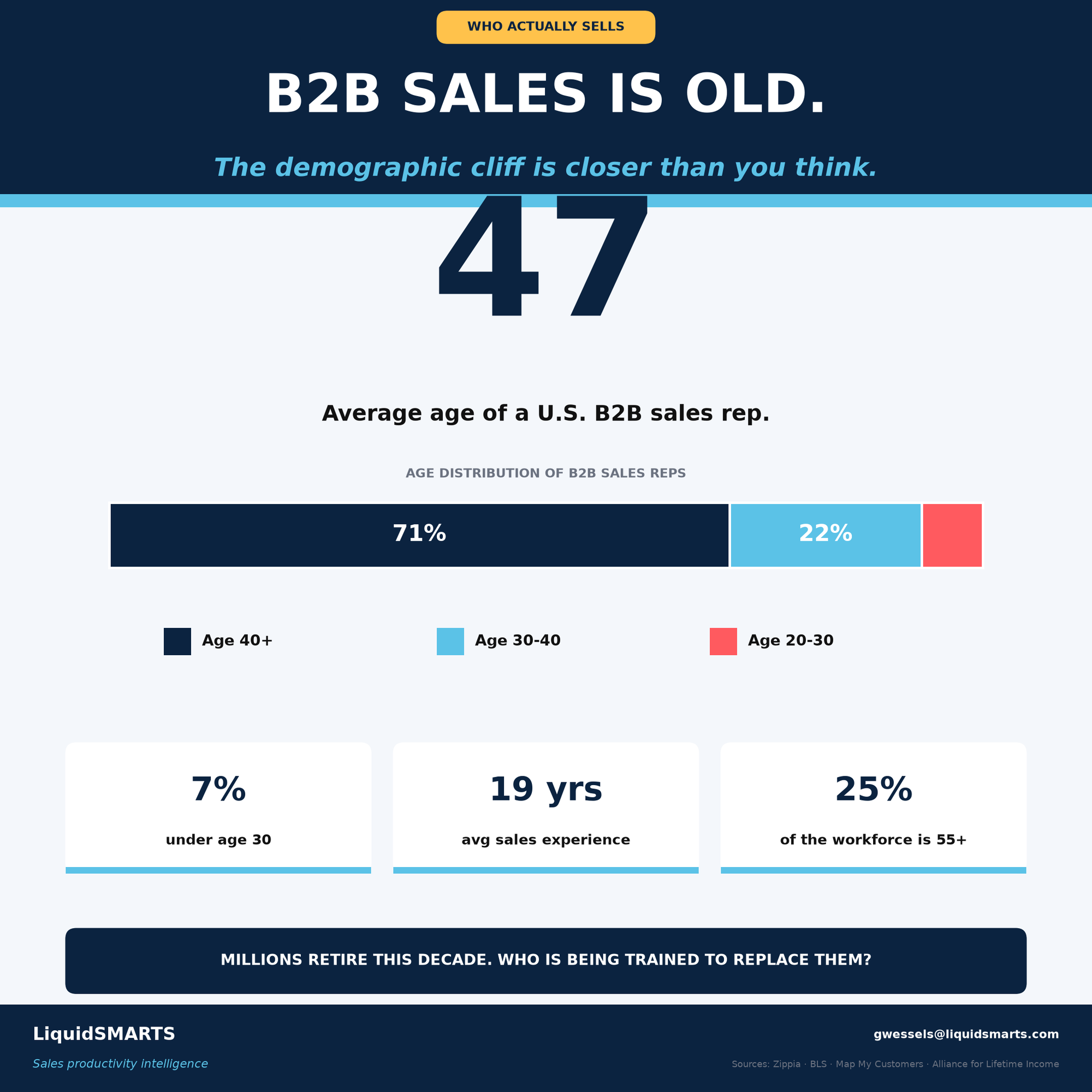
Average age 47. Average experience 19 years. Twenty-five percent of the workforce is 55 or older. Zippia puts the average medical sales specialist at 47 as well.
The people who know how to get into an OR, hold a surgeon's attention through a difficult case and defend a price to a value analysis committee are, as a population, closer to retirement than to their next promotion. There is no bench. The industry spent a decade optimizing quarterly attainment and never staffed the succession of its own most valuable skill.
And the job is getting harder in ways that have nothing to do with the rep.
| Force | The number | What it does to the rep |
|---|---|---|
| Procedures moving to ASCs | 65% of US surgeries now in ASCs | The buying decision leaves the hospital relationships you spent 15 years building |
| Vendor credentialing | 90% of facilities require it, $300 to $800/yr per system | Access is now a cost center and a gate |
| Tariffs | Section 232 device investigation opened Sept 2025, action possible summer 2026 | Boston Scientific already absorbed roughly $200M in 2025 exposure |
| OEM restructuring | Intuitive cut 331 at HQ. Medtronic closing Santa Rosa. Zeiss shedding up to 1,000 | Territories get redrawn by people who have never met you |
| Category exits | Boston Scientific left TAVR entirely, May 2025 | An entire book of business, gone by memo |
So the ladder is real, the ceiling is real, and the ground is moving.
What You Sell Is Really When You Joined
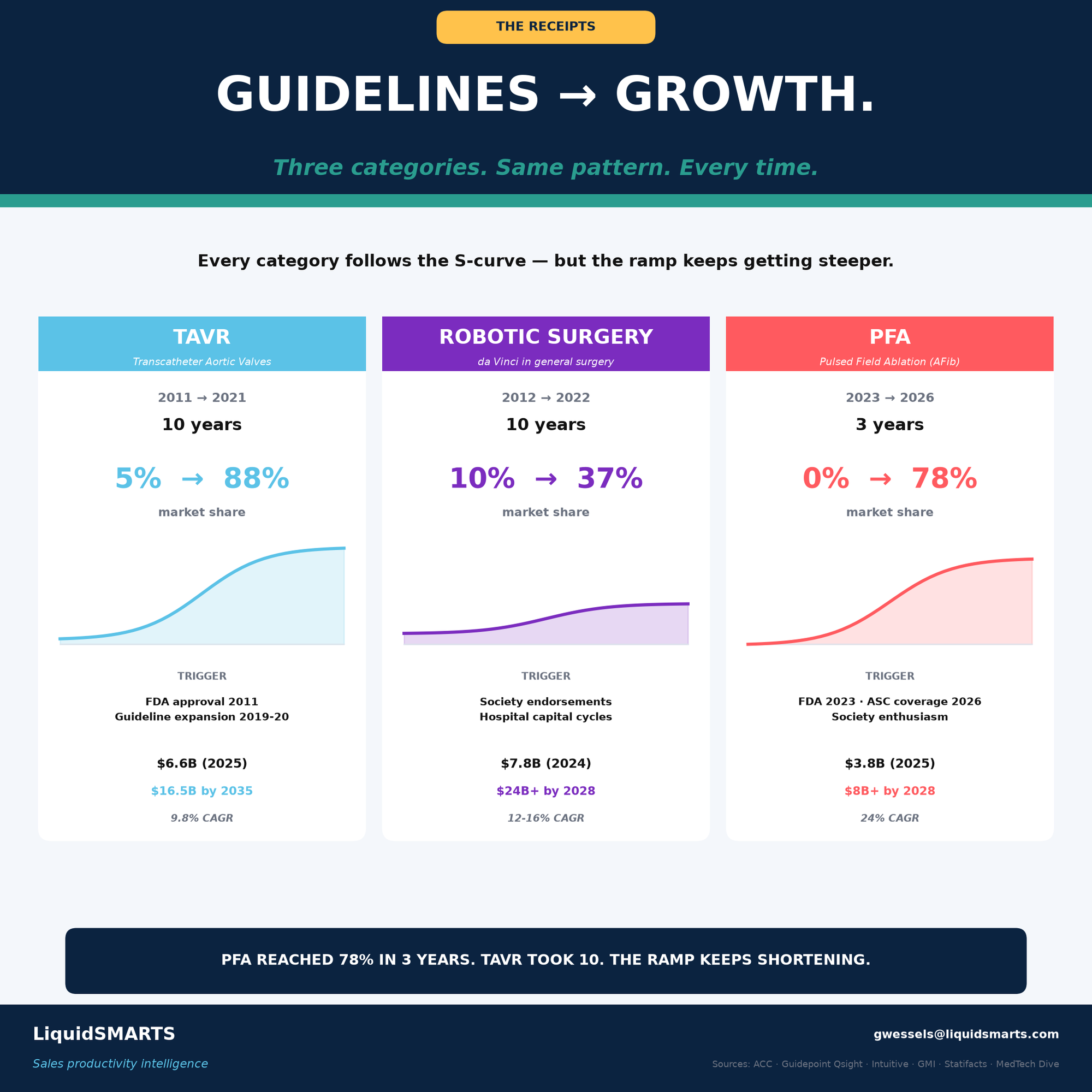
Every device category follows an S-curve, and the ramp keeps getting steeper.
| Category | Window | Duration | Market share | CAGR |
|---|---|---|---|---|
| TAVR | 2011 to 2021 | 10 years | 5% to 88% | 9.8% |
| Robotic surgery | 2012 to 2022 | 10 years | 10% to 37% | 12 to 16% |
| Pulsed field ablation | 2023 to 2026 | 3 years | 0% to 78% | 24% |
TAVR took ten years to do what PFA did in three.
Now overlay rep earnings on that curve and you get the finding that reframes the whole career.
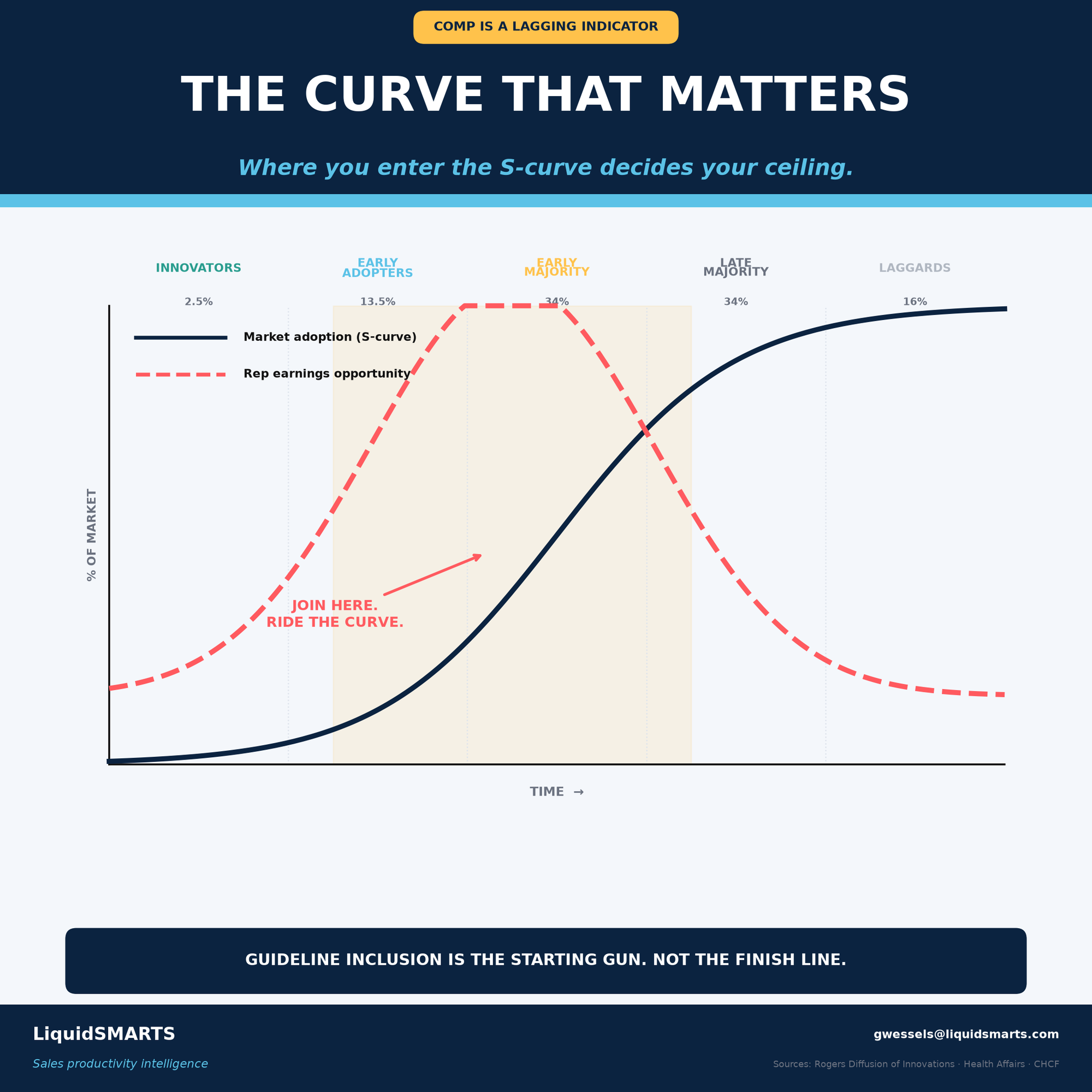
Earnings opportunity does not track market share. It peaks in the early adopter band, roughly the 13.5 percent of the market that moves after the innovators and before the early majority, and then it decays through late majority even as the category keeps growing.
The reason is not mysterious. In the early band you are selling a decision. The territory is unworked, the quota is set from guesswork rather than history and the accelerators are uncapped because nobody has modeled what a great year looks like yet. By late majority you are defending share against three competitors on a GPO contract in front of a value analysis committee that has seen your deck twice.
| Stage | Share of market | Rep earnings opportunity |
|---|---|---|
| Innovators | 2.5% | Low. No budget, no code, no volume |
| Early adopters | 13.5% | Peak. Unworked territory, soft quota, uncapped accelerators |
| Early majority | 34% | Declining. Quota catches up to reality |
| Late majority | 34% | Low. Price defense on contract |
| Laggards | 16% | Floor. Renewal and service |
The $600K spine rep and the $125K imaging rep are running the same play at different points on the same curve.
Compensation is a lagging indicator of a position decision made years earlier. Usually not by the rep. Usually not deliberately by anyone.
Guideline inclusion is the starting gun, not the finish line. That is the part reps read backwards. They see a category earn a guideline and a CMS coverage decision, conclude the opportunity is confirmed and therefore safe, and join. By then the earnings curve has already peaked. The money was in the eighteen months before the confirmation, when the thing still looked risky.
Coaching Is Positioning. Training Is Skill.
Here is where this turns, and it is the argument I most want you to take away.
The industry has collapsed two different jobs into one word. We say "coaching" when we mean "training," and then we wonder why the coaching does not move the number.
Training builds capability inside the rep. Product knowledge. Objection handling. The call plan. Discovery questions. How to run a value analysis committee meeting. Training answers one question: can this rep execute the play? It is teachable, it is testable and it belongs in a curriculum with a mastery gate. We build those for a living and they work.
Coaching decides where that capability gets pointed. Which category. Which accounts. Which curve. Which rep gets the launch bag and which one gets the mature line. When someone is ready to be moved and, more to the point, when they are not. Coaching answers a different question: is this rep positioned where their capability compounds?
A rep can be perfectly trained and badly positioned. That rep will work sixty hours a week defending late-majority share on a GPO contract, hit 80 percent of quota, and their manager will put them on a skills plan.
That is the coaching gap. Not a deficit of technique. A deficit of positioning.
And the data proves it twice.
Proof one. The SDR clock.

| Promoted to AE at | AE failure rate |
|---|---|
| Under 11 months | 55% |
| 16+ months | 6% |
| Comp lift on promotion | 50 to 80% |
| Annual SDR turnover | 34% |
Same person. Same talent. Same ambition. Different clock, and a nine-times difference in outcome.
Nobody fails at 55 percent because they lack skill. They fail because a manager made a positioning decision at month nine that felt like a reward. The promotion is real, the comp lift is real, and it is the single most reliable way to end a promising career, because the rep gets moved before the reps are learned, misses number in the first two AE cycles and carries an AE failure on the record instead of an SDR success.
Patience is the highest-return coaching skill in sales and it appears on no competency model I have ever been handed.
Proof two. The allocation of your best cohort.
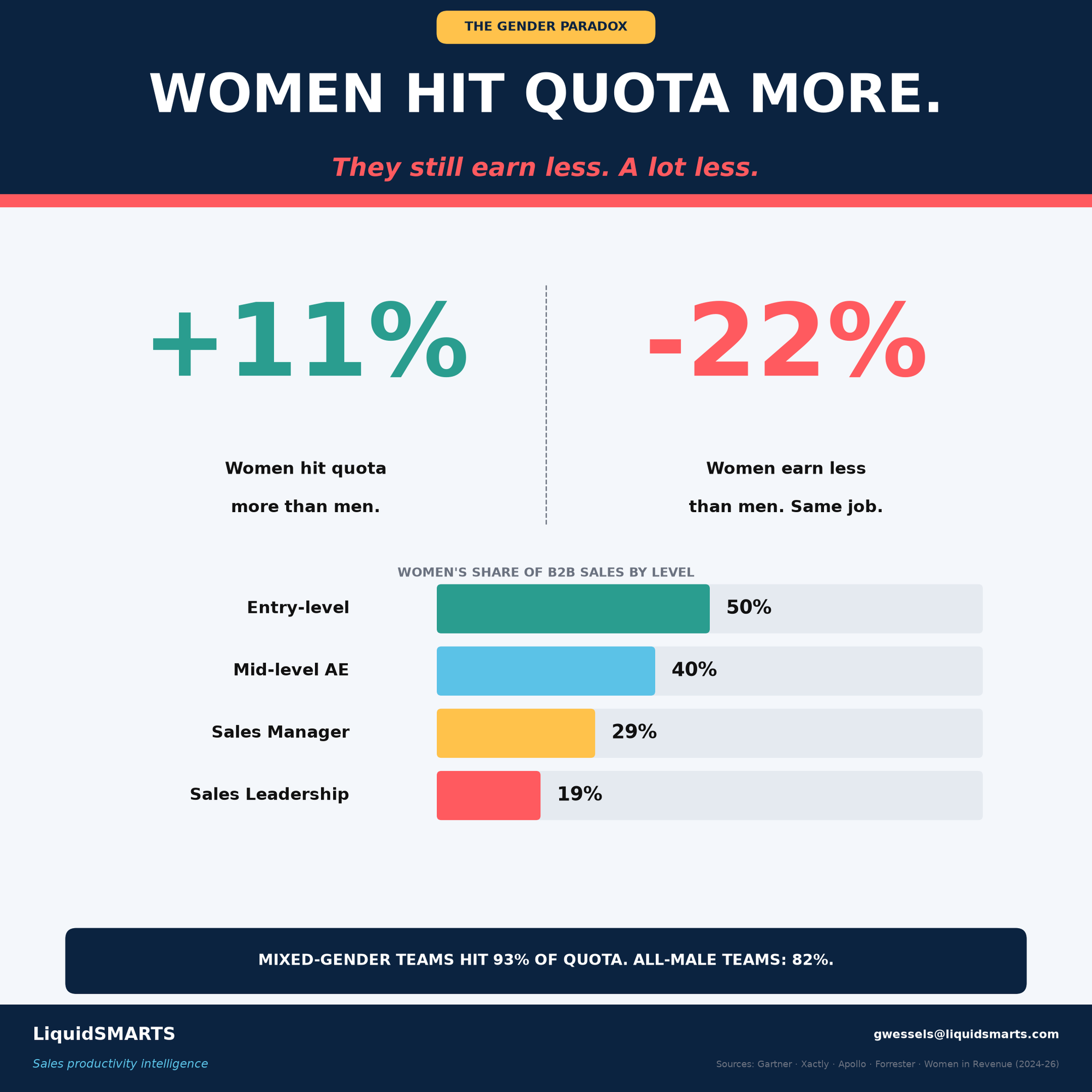
| Level | Women's share of B2B sales |
|---|---|
| Entry level | 50% |
| Mid-level AE | 40% |
| Sales manager | 29% |
| Sales leadership | 19% |
Women hit quota 11 percent more often than men. They earn 22 percent less for the same job. Mixed-gender teams hit 93 percent of quota. All-male teams hit 82 percent.
The usual framing here is fairness and the usual response is a values statement. That is not the argument I am making. Look at it as positioning.
The highest-attainment cohort in the industry is being routed away from the highest-ceiling curves. Every one of those percentages is a decision somebody made about who gets the spine bag, who gets the robotics launch, who gets the PFA territory in year one. If your best-attaining population is underrepresented in the categories where money compounds, you do not have a diversity gap. You have a talent misallocation, and it is showing up in your own attainment number. The 93 versus 82 is right there in the data.
Training cannot fix either of those failures. No curriculum reaches them. They are both positioning, and positioning is the coach's job.
The Things You Would Expect to Matter, Do Not
Now the part that annoys people, and should.

| Level | Share | Average salary |
|---|---|---|
| Bachelor's | 67% | $71,753 |
| Associate / some college | 15% | $59,645 |
| High school or less | 8% | $57,925 |
| Master's | 7% | $78,069 |
A master's buys about $6,300 a year over a bachelor's. Moving from diagnostic imaging to spine buys $175,000 a year in average OTE and swings the ceiling by nearly $400,000.
The degree is worth roughly three percent of what the position is worth. This is the last un-credentialed six-figure career path in the American economy, and the industry keeps screening for a diploma its own compensation data says is close to irrelevant.
Tenure matters more, and it saturates.
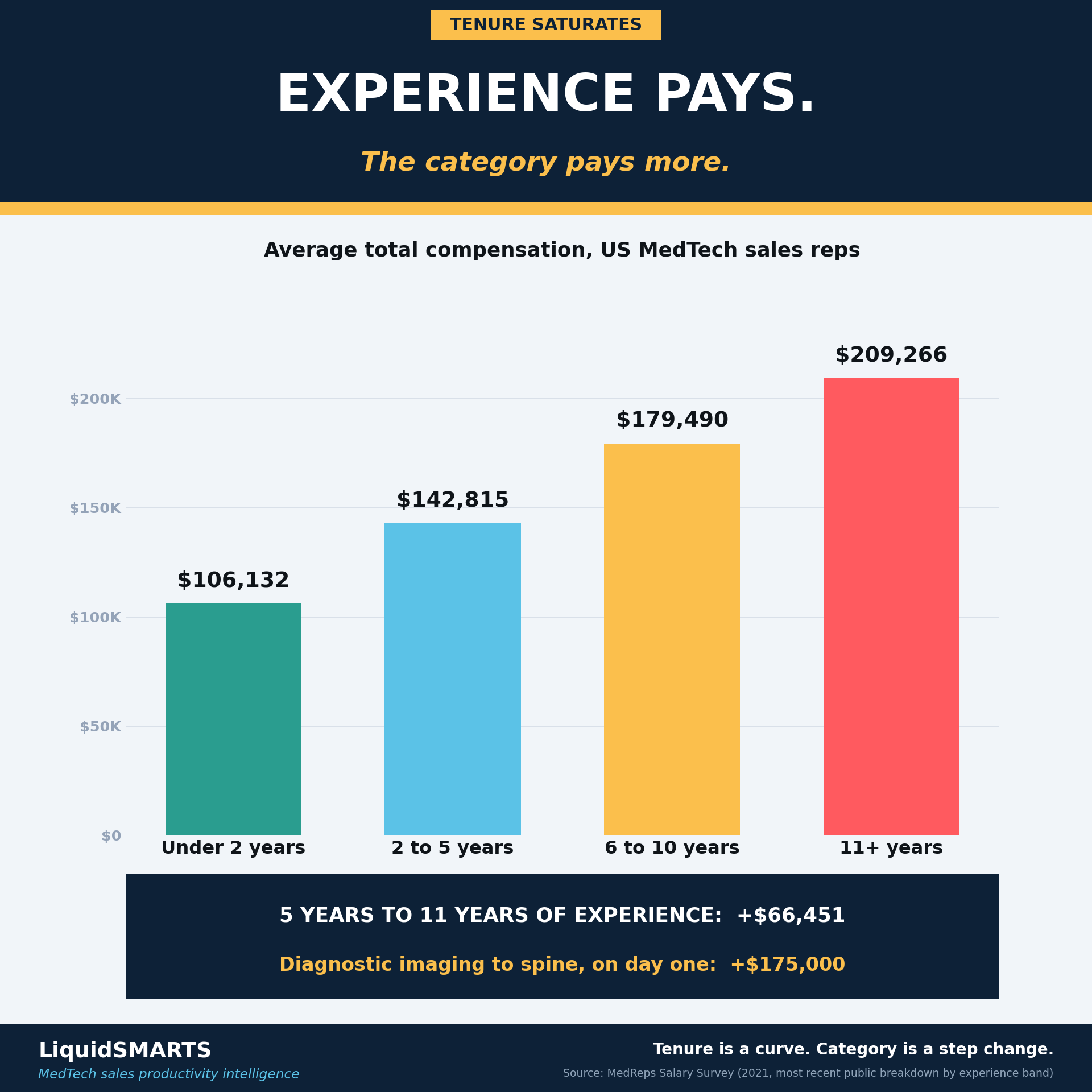
| Experience | Total comp |
|---|---|
| Under 2 years | $106,132 |
| 2 to 5 years | $142,815 |
| 6 to 10 years | $179,490 |
| 11+ years | $209,266 |
That is a real curve, and the underlying MedReps survey is 2021 data, so treat the levels as dated and the shape as sound. Doubling experience from five years to eleven adds about $66,000. Being on the right curve adds three times that.
Effort does not save you either.
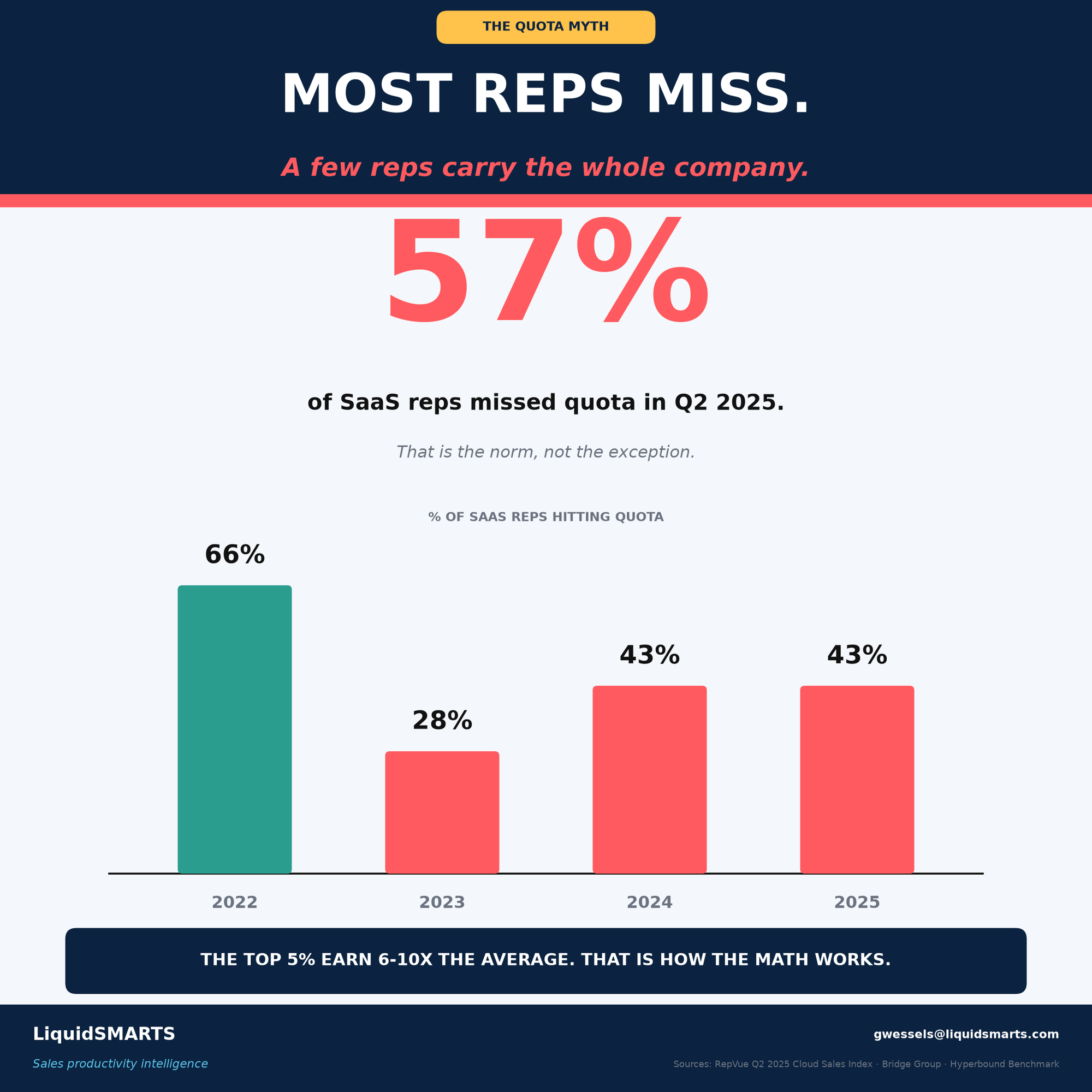
| Year | Attainment |
|---|---|
| 2022 | 66% |
| 2023 | 28% |
| 2024 | 43% |
| 2025 | 43% |
Fifty-seven percent of reps missed quota in Q2 2025. The median rep now misses. That is not a performance crisis, it is a quota-setting decision, and it is why the top 5 percent earn six to ten times the average. The distribution is built that way on purpose.
The Number That Does Not Reconcile, and Why I Am Telling You
Two of these datasets disagree, and I would rather name it than quietly pick the flattering one.
Glassdoor's blended average for a medical device rep is $157,251, with a 90th percentile of $266,054. RepVue's blended median OTE is $170,000 with top performers at $374,120. Both sit well below the specialty averages of $175,000 to $300,000 in the first table.
They measure different populations. The blended figures include every device sales title at every level, including entry-level consumables and disposables reps with no OR responsibility, who start around $63,000. The specialty figures are OR-dependent, implant-heavy, commission-loaded categories staffed mostly by mid-career reps. The BLS median for the closest government occupation code is $100,070, and that code also covers industrial and scientific instrument reps, so it is useful for sizing the workforce and useless for pricing a spine rep.
The gap between $63,000 and $600,000 is not a data error. It is the career. It is everything that happens between the first bag and the right bag, and the industry does almost nothing to help a rep cross it deliberately.
The Move
This week, run a position audit. On yourself, and on every rep you manage. Four questions, one page, thirty minutes.
Where is my category on the S-curve? Innovators, early adopters, early majority, late majority, laggard. Be honest. If the product has been in the guidelines five years and three direct competitors sit on the same GPO contract, you are in late majority and the earnings curve is descending no matter how hard the territory gets worked.
What repriced my territory in the last 24 months, and what reprices it in the next 18? A guideline revision, a CMS coverage decision, an ASC payment rule, a competitor's exit. Boston Scientific leaving TAVR in May 2025 changed somebody's year. Name the decision, the body that makes it and the approximate date.
Am I positioned for where the volume is going? Sixty-five percent of surgeries are now in ASCs. If the entire relationship map is hospital-based and the entire access model assumes an OR badge at an IDN, that is optimization for where the volume was.
If I were joining today, would I join my own category? This one stings. If the answer is no, you have your answer, and the data says the window on the next curve is shorter than the last one was.
Then look at where the curves are inflecting right now.

| Category | Trigger | Stage |
|---|---|---|
| Pulsed field ablation | FDA 2023, ASC coverage Jan 2026 | Early majority |
| Renal denervation | ACC/AHA guideline Aug 2025, CMS coverage Oct 2025 | Early adopter |
| Structural heart beyond TAVR | Mitral, tricuspid, valve-in-valve entering guidelines | Early majority |
| GLP-1s in cardiometabolic | CV outcome trials, CMS coverage expanding | Early majority |
| Point-of-care ultrasound | AIUM 2025 credentialing update | Early adopter |
Reps hired into those categories in 2024 and 2025 will earn in 2029 the way TAVR reps earned in 2015.
For the leaders, the audit is the same and the stakes are different. Your best-attaining reps are underrepresented in your highest-ceiling categories. Your median rep is missing quota by design. Your average rep is 47 and there is nobody behind them.
You cannot train your way out of any of that. Training is what you do once the rep is in the right seat. Deciding the seat is the job, and it is the one most managers never make explicit.
So stop coaching technique to a rep who is standing on the wrong curve. Move the rep.
One page. Four questions. The position you hold is worth more than the degree you earned, the years you served or the hours you put in. Pick the curve, then train like hell on it.
Sources: MedReps, RepVue, SLR Medical, Everstage, Glassdoor (2025-26). BLS Occupational Outlook Handbook, SOC 41-4011 (2024, projections to 2034). Zippia B2B sales rep demographics. Gartner, Xactly, Apollo, Forrester, Women in Revenue (2024-26). Bridge Group, Prospeo, Skipcall. RepVue Q2 2025 Cloud Sales Index. AdvaMed and Frost & Sullivan. Precedence Research and Coherent Market Insights (ASC). MedTech Dive and MassDevice (tariffs, restructuring). ACC, AHA, CMS, AIUM, Rogers Diffusion of Innovations.
Dr. Gunter Wessels is the founder of LiquidSMARTS℠, a commercial engineering firm for medical technology companies. LiquidSMARTS℠ guarantees a 10% pipeline velocity improvement in 90 days.